"For decades, CHS was invisible. Not because it did not exist, but because no one was looking for it. Understanding where it comes from is the first step to being believed."
CHS Patient Community- ▸ CHS was first formally described in medical literature in 2004. It is not a new condition, just newly recognized.
- ▸ Estimated to affect 2–3 million people in the U.S. alone, though most cases go undiagnosed.
- ▸ Rising prevalence correlates directly with higher-potency cannabis and increased long-term use.
- ▸ No single "CHS gene" has been identified, but genetic susceptibility is strongly suspected.
- ▸ CHS is frequently mistaken for cyclic vomiting syndrome (CVS), gastroparesis, and other GI conditions.
A Modern Diagnosis: The 2004 Discovery
Cannabinoid Hyperemesis Syndrome was first described in a landmark 2004 paper by Allen et al., published in Gut, a peer-reviewed gastroenterology journal. The study documented a cluster of patients in South Australia who shared the same baffling pattern: years of heavy cannabis use, recurrent episodes of severe vomiting, and one peculiar relief behavior: compulsive hot bathing.
Before 2004, these patients were cycling through emergency rooms and specialist offices without answers. Many were labeled as having "functional" GI disorders or psychosomatic illness. The 2004 paper named the syndrome for the first time and established its three hallmark phases: prodromal, hyperemetic, and recovery.
What the 2004 paper could not explain, and what researchers are still working to understand, is why it happens to some heavy cannabis users and not others. That question points directly to genetics.
The Iceberg of Prevalence
CHS is what epidemiologists call an "iceberg condition." The visible tip (confirmed diagnoses) represents only a fraction of actual cases. Beneath the surface lies a vast population of people who are:
- Misdiagnosed: labeled with CVS, gastroparesis, functional nausea, or anxiety disorders.
- Unaware: actively using cannabis and not yet connecting it to their symptoms.
- Avoiding care: hesitant to disclose cannabis use to healthcare providers due to stigma or legal concerns.
- Dismissed: seen in ERs where CHS is not on the differential, treated symptomatically, and discharged.
A 2018 analysis published in Basic & Clinical Pharmacology & Toxicology estimated that up to 6% of people who visit emergency rooms for vomiting may have CHS, a staggering proportion given how rarely the diagnosis is made on first presentation.
Why CHS Cases Are Rising
CHS prevalence is not simply growing because doctors are better at finding it. Multiple converging factors are driving a genuine increase in cases:
- Higher potency cannabis: THC concentrations have risen from roughly 4% in the 1990s to 12–25%+ in flower and up to 90%+ in concentrates. The cumulative receptor load is dramatically higher.
- Earlier onset of use: Adolescent use means longer lifetime exposure by the time symptoms emerge in a person's 20s or 30s.
- Normalization and legalization: Reduced social stigma has led to more open daily use, precisely the pattern most associated with CHS development.
- Concentrate and edible culture: Dabbing, vaping, and high-dose edibles deliver acute THC loads that may overwhelm receptor regulation more rapidly than traditional smoking.
- Longer use duration: CHS typically requires years of heavy use to manifest. As legalization expands the population of long-term heavy users, CHS incidence follows.
The Genetic Question
The most confounding aspect of CHS is selectivity: millions of people use cannabis heavily for years without developing the syndrome. This strongly suggests an underlying genetic or biological vulnerability. While no definitive "CHS gene" has been identified, researchers have proposed several mechanisms:
🔬 CB1 Receptor Variants
Polymorphisms in the CNR1 gene (which encodes the CB1 receptor) may alter how the endocannabinoid system responds to chronic THC exposure, potentially driving dysregulation in the hypothalamus and gut.
⚙️ CYP Enzyme Differences
Variations in cytochrome P450 enzymes (particularly CYP2C9 and CYP3A4) affect how quickly THC and its metabolites are processed. Slow metabolizers may accumulate THC metabolites at levels that disrupt GI motility.
🌡️ TRPV1 Thermosensitivity
The TRPV1 receptor (activated by heat) is closely linked to nausea and the hot-shower relief behavior in CHS. Genetic differences in TRPV1 expression or sensitivity may explain both symptom presentation and the paradoxical heat response.
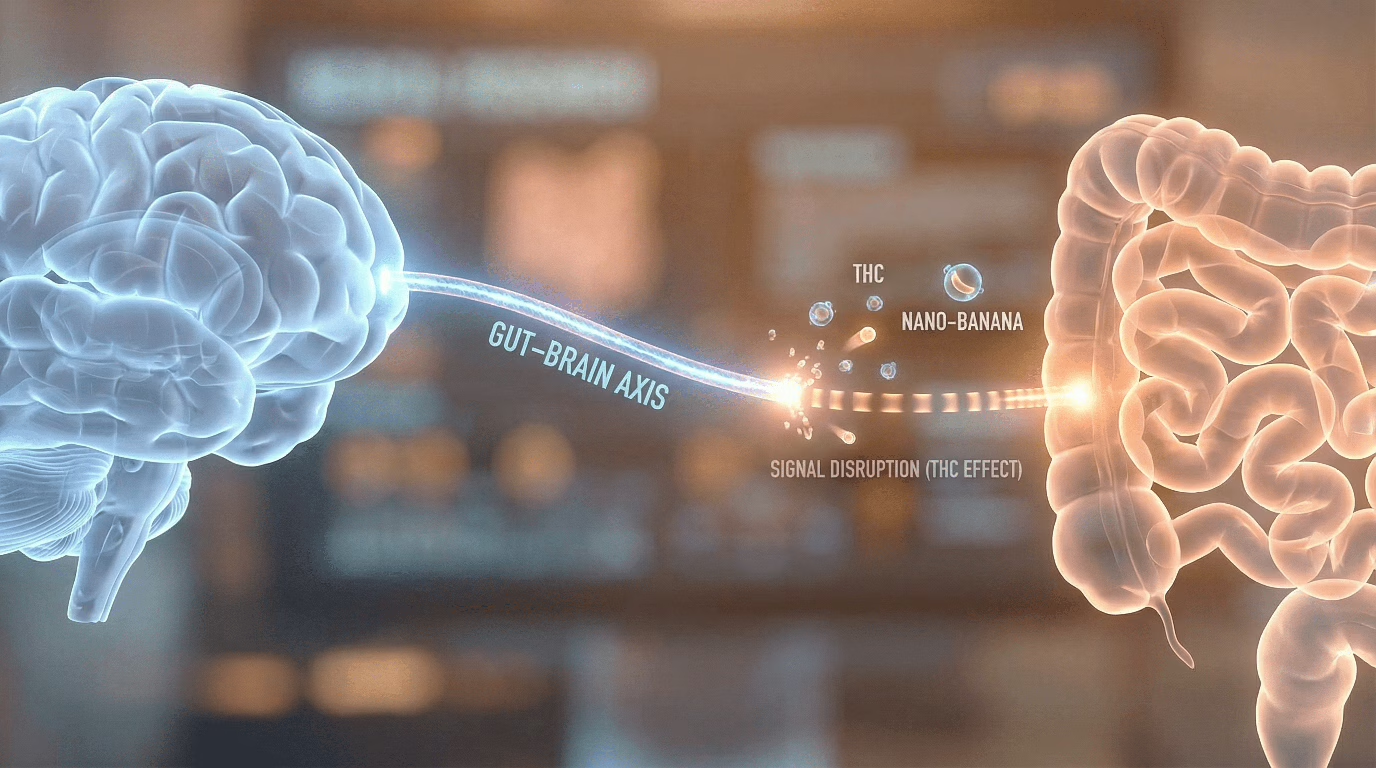
🧠 Hypothalamic Dysregulation
Chronic high-dose THC may gradually alter hypothalamic temperature and nausea regulation. Those with genetic predisposition toward certain neuroendocrine baselines may reach this tipping point sooner.
Research into CHS genetics is still early-stage. Most studies are retrospective case series rather than prospective genomic investigations. As CHS gains wider recognition, and as biobanks grow, large-scale genetic association studies are becoming feasible and are increasingly being called for by researchers in the field.
CHS vs. The Impostors
CHS shares symptoms with several other conditions, which is why it is so frequently misdiagnosed. Here is how it differs from the most common diagnostic alternatives:
Frequently Asked Questions
Q If cannabis is known to help nausea, why does it cause CHS?
Acute or low-dose cannabis does act as an antiemetic; this is why it is used in chemotherapy patients. However, with chronic high-dose exposure, the endocannabinoid system undergoes desensitization and downregulation. The same receptors that normally suppress nausea begin to function abnormally, ultimately triggering the opposite response. CHS represents a system that has been pushed past its regulatory limits.
Q Can someone be genetically tested to know if they are at risk for CHS?
Not yet. There is currently no validated clinical genetic test for CHS susceptibility. While researchers have identified several candidate genes and pathways, none have been confirmed with sufficient evidence to form the basis of a diagnostic test. This remains an active area of research and an important unmet need in the field.
Q Does CHS mean I will always be sensitive to cannabis, even after recovery?
The current clinical evidence strongly suggests yes. The overwhelming majority of patients who resume cannabis use after CHS remission experience a return of symptoms, often more quickly than the original onset. This pattern is consistent with a persistent underlying vulnerability rather than a temporary physiological state. Most CHS specialists advise permanent abstinence as the only reliable long-term solution.











{kind=link}